Hereditary Macrothrombocytopenias and Impact-R
Wednesday, December 14th, 2011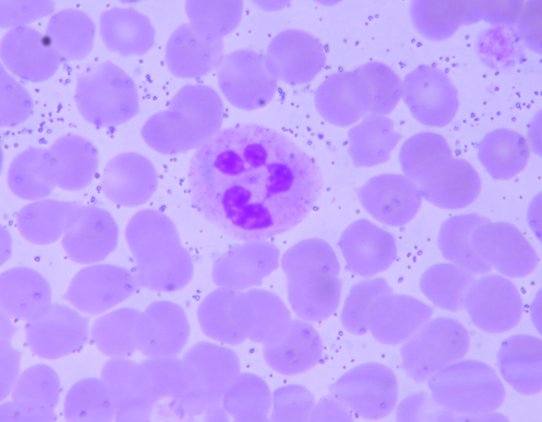
Dohle body in the cytoplasm of a granulocyte.
The Inherited Macro-thrombocytopenias are autosomal dominant disorders characterized by mild to moderate thrombocytopenia with large platelets and varying degrees of platelet dysfunction, usually an absence or reduction of the secondary wave of platelet aggregation resulting in little or no bleeding. Thrombopenic symptoms are purpura, ecchymoses, epistaxis and heavy menstrual bleeding. Some may also have leukocyte inclusions, interstitial nephritis, sensorineural hearing loss and cataracts. Mutations in the heavy chain IIA MYH9, a prominent non-muscle myosin, result in a spectrum of disorders with variable manifestations.
May-Heggelin anomaly (MHA) is characterized by macrothrombocytopenia and presence of Döhle bodies in the cytoplasm of leukocytes. Most of the time, MHA requires no treatment but in extreme cases, a platelet transfusion may be beneficial.
Fechtner syndrome includes a macrothrombocytopenia with smaller calibre platelets than MHA, leukocyte inclusions, interstitial glomerulonephritis, sensorineural deafness, and cataracts. Treatment includes specific management of the components (e.g. lens replacement for cataract) and platelet transfusions if contemplating surgery.
Sebastian syndrome is purely hematologic in manifestation. It involves macrothrombocytopenia which is usually asymptomatic and leukocyte inclusion bodies that are smaller than those seen in MHA, may be numerous and are generally difficult to stain.
Epstein syndrome has nephritis, hearing loss, platelet adhesion and aggregation defects but no leukocyte inclusions are demonstrated. Eckstein syndrome has nephritis and deafness but no platelet dysfunction. Enyeart syndrome has thrombocytopenia and giant platelets with inclusions but no leukocyte inclusions.
Cytoplasmic inclusions are formed when the unstable abnormally dimerized MYHIIA protein precipitates with the normal MYHIIA.
Giant platelet.
Abnormal dimerization also brings about failure to properly organize the cytoskeleton of megakaryocytes, which causes giant platelets and thrombocytopenia.
Since these disorders are autosomal dominant with phenotypic consequences that are not readily apparent, screening tests for siblings or offspring of known affected individuals may be an important step. In this regard, Impact-R can be of much use. It is a cone and platelet analyzer that qualitatively determines platelet adhesion and aggregation. A peripheral smear alone may not predict the need for platelet transfusions in patients about to undergo surgery. Impact-R could also be of much use in further research for these conditions especially in answering the question, “How is adhesion and aggregation affected by abnormal platelet size?”